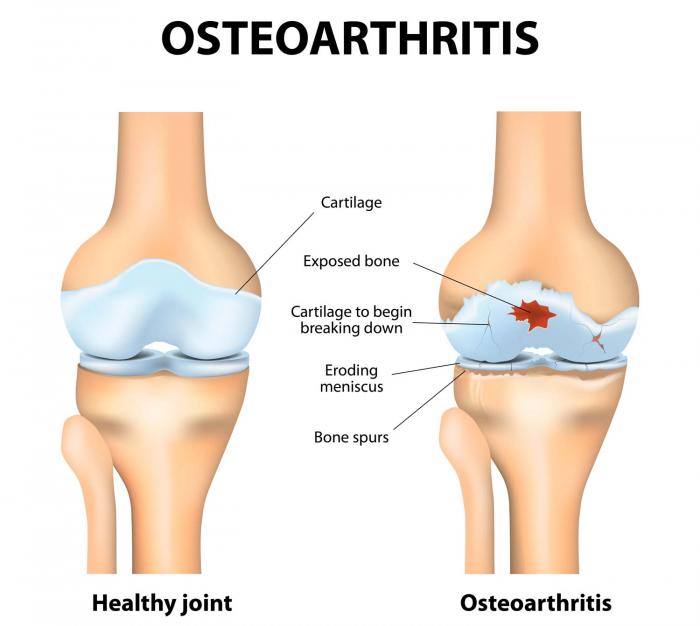
Knee osteoarthritis (OA) is a very common condition caused by degeneration of the cartilage in the knee joint. It can be a very painful condition and we see many clients in the clinic suffering from it. When I sat down to write this blog, I wanted to learn more about what the research shows to be effective in treating it and I wanted to get an expert’s opinion. I was lucky enough to be able to ask Dr Tony Kostos, an extremely experienced and well respected rheumatologist who is based in East Melbourne.
What do Rheumatologists do?
Rheumatologists are expert physicians who assess and treat many different arthritic, musculo-skeletal and auto-immune diseases. Your GP may refer you to see a rheumatologist if you have any of the following conditions:
- Osteoarthritis
- Gout
- Osteoporosis
- Ongoing pain without a diagnosis
- Fibromyalgia
- Rheumatoid Arthritis
- Psoriatic Arthritis
- Anklyosing Spondylitis
- Reactive Arthritis
- Lupus
- Scleroderma
- Sjogren’s Syndrome
- Myositis
I sat down with Dr Kostos and asked the following questions.
What is the most effective treatment for knee osteoarthritis?
We recommend conservative treatment with exercise and weight loss in particular, and occasional anti inflammatory medication
A knee arthroscope (keywhole surgery that can involve washing and cleaning out the joint) seems to be a common treatment choice. Dr Kostos, please tell me if the evidence indicates this is an effective treatment?
There have now been 13 studies dating back to 2002 comparing knee Arthroscopy with sham surgery, physiotherapy and exercise in patients with osteoarthritis and patients with degenerative meniscal tears with and without osteoarthritis. This includes patients with locking of the knee, the symptom that orthopaedic surgeons insist is the main indication for Arthroscopy. None of these studies have shown any benefit of Arthroscopy.
What about other non-conservative treatments?
There is insufficient evidence for glucosamine (natural sugar reported to build cartilage), chondroitin (natural substance reported to draw water and nutrients into cartilage), blood PRP (platelet rich plasma) and stem cell injections.
Dr Kostos, what is your opinion on clinical pilates?
Clinical Pilates is an excellent way of targeting problem areas and importantly is also fun.
So, in summary, if you have knee osteoarthritis and you are experiencing pain, please ensure you book in with your physiotherapist for an assessment where we can prescribe safe and suitable exercises and chat about starting clinical pilates to improve your pain. If you have any of the conditions listed above and feel you are not improving, please speak to your GP about a rheumatology referral.
And a special thanks to Dr Tony Kostos for taking the time to help us learn more about the effective treatment of knee osteoarthritis.
- Julia Esposito